
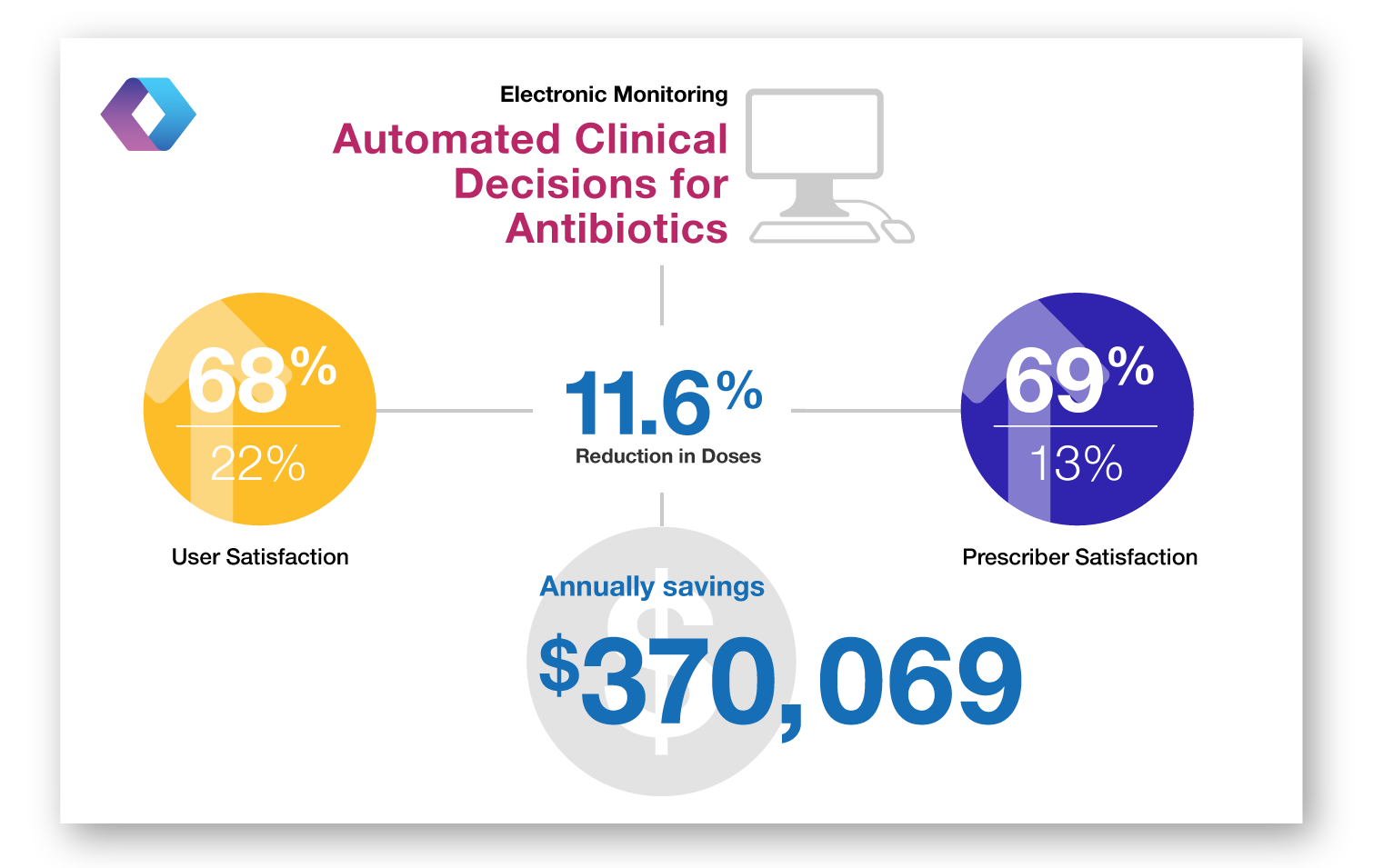
A World Wide Web-based antimicrobial stewardship program improves efficiency, communication, and user satisfaction and reduces cost in a tertiary care pediatric medical center.
Electronic Monitoring – Implementation of a web-based program to provide automated clinical decision support, faciliate approval and real-time communication with prescribers related to antibiotics.

Enforcing a policy for restricting antimicrobial drug use
Restriction – Eight IV antibiotics (amikacin, aztreonam, ceftazidime, ciprofloxacin, fluconazole, imipenem-cilastatin, ofloxacin, and ticarcillin-clavulanate, (aztreonam was added to list two months into intervention) previously needed approval, but enforcement of restrictions lax. All staff informed that ID approval needed for dispensement and that pharmacists needed to be informed in writing or by telephone. Enhanced enforcement included issuing warnings to pharmacists if restricted antibiotics dispensed without ID approval.

Impact of a computerized clinical decision support system on reducing inappropriate antimicrobial use: A randomized controlled trial
Electronic Monitoring – randomized controlled trial of active monitoring by antimicrobial management team of all restricted antibiotic orders with a computer system compared to a group without the computer system to alert for inadequate antimicrobial therapy.

Early transition to oral antibiotic therapy for community-acquired pneumonia: duration of therapy, clinical outcomes, and cost analysis
Conversion – CAP pts randomized to conventional course of IV antibiotics vs. abbreviated course of IV antibiotics followed by conversion to oral antibiotics conversion-CAP pts randomized to conventional course of IV antibiotics vs. abbreviated course of IV antibiotics followed by conversion to oral antibiotics.

A pharmacist-initiated program of intravenous to oral antibiotic conversion
Conversion – Pharmacists contacted physicians to recommend oral antibiotics conversions from selected broad-spectrum and high-cost parenteral antibiotics for patients with predetermined mild to moderate clinical conditions.

Cost-effectiveness of prospective and continuous parenteral antibiotic control: experience at the Palo Alto Veterans Affairs Medical Center from 1987 to 1989
Multidisciplinary – Implementation of new restrictions in antibiotic formulary for broad-spectrum antibiotics and restrictions for antibiotics maximum daily dosage.

Reduction of incorrect antibiotic dosing through a structured educational order form.
Order form – Creation of an order form with preset dosing orders for clindamycin, cefazolin and metronidazole. Physicians still had option to choose own dosing schedule on the form.

Antibiotic cost savings from formulary restrictions and physician monitoring in a medical-school-affiliated hospital
Restriction-creation of formulary restrictions for vancomycin and select aminoglycocides and cephalosporins, which would require obtaining ID approval for use. ID told not to reject requests but to use persuasion.

Controlling cephalosporin and aminoglycoside costs through pharmacy and therapeutics committee restrictions
Guidelines – Established restrictions on use of 2nd generation cephalosporins and aminoglycosides requiring obtaining pharmacy approval before drug disbursement

Reduction in antibiotic costs by restricting use of an oral cephalosporin
Restriction-All physicians wanting to prescribe cephalexin had to seek approval from ID physician.

Cost containment through restriction of cephalosporins
Guidelines – Establishment of guidelines that cefazolin is cephalosporin of choice. Physicians contacted if orders deemed to be noncompliant.